




What Is Sciatica?
Sciatica is an outdated and often misunderstood term. To most people, it simply means “pain in the leg that comes from the back.” However, sciatica is an umbrella term and it’s a word used to describe a group of symptoms, not the underlying cause.
When someone says they have sciatica, they’re usually referring to one of the following:
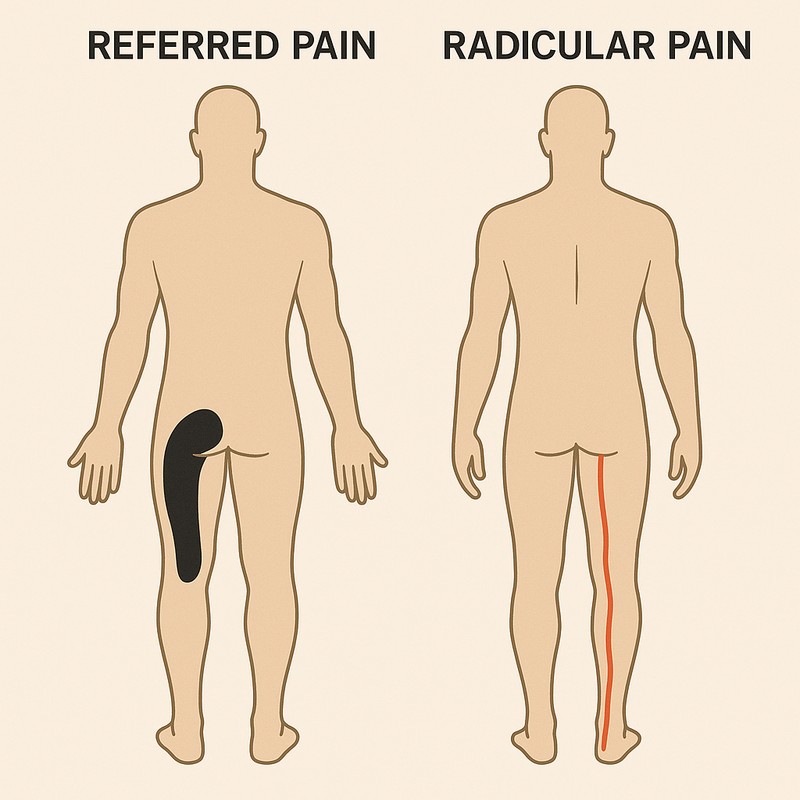
- Radicular pain – Sharp, burning pain caused by inflammation or compression of a spinal nerve root, often linked to a disc herniation.
- Radiculopathy – Nerve dysfunction that may include numbness, weakness, or loss of reflexes, also due to nerve root involvement.
- Referred pain – The most common of the three. This pain travels down the leg but originates from irritated structures in the back, without direct nerve involvement. Involving nerves other than those that supply the original injury (Bogduk, 2009).
Most people who believe they have sciatica are referring to radicular pain or radiculopathy, but it’s common to be misdiagnosed when the issue is actually referred pain.
What Causes Sciatica?
Sciatica is more accurately described as nerve root irritation or compression. It is typically caused by two main factors:
- Mechanical pressure from surrounding structures: Most often from disc material or other tissues reducing the space around the nerve root.
- Chemical irritation: Inflammatory substances released by damaged tissues (such as the facet joint) can irritate the nerve, even in the absence of significant compression (Peng et al., 2007).
Common sources of pain:
- Disc material: causing compression, stretching, and/or chemical irritation of the nerve.
- Surrounding structures: facet joints can leak inflammatory substance into the nerve root causing symptoms.
- Stenosis: compression from a narrowing of the areas where nerves exit the spine.
Do I Need a Scan to Diagnose?
Not always.
Scans (like MRIs) can be helpful, but only in specific situations such as:
- Lack of improvement
- Signs of serious pathology (red flags)
- When imaging would change the treatment approach
For most people, a clinical diagnosis based on history and physical testing is sufficient. Scans rarely change the actual rehab plan.
Why Scans Can Be Misleading
It’s a common belief that a scan shows exactly what’s wrong. Scans often reveal age-related changes that are also seen in people with no symptoms at all.
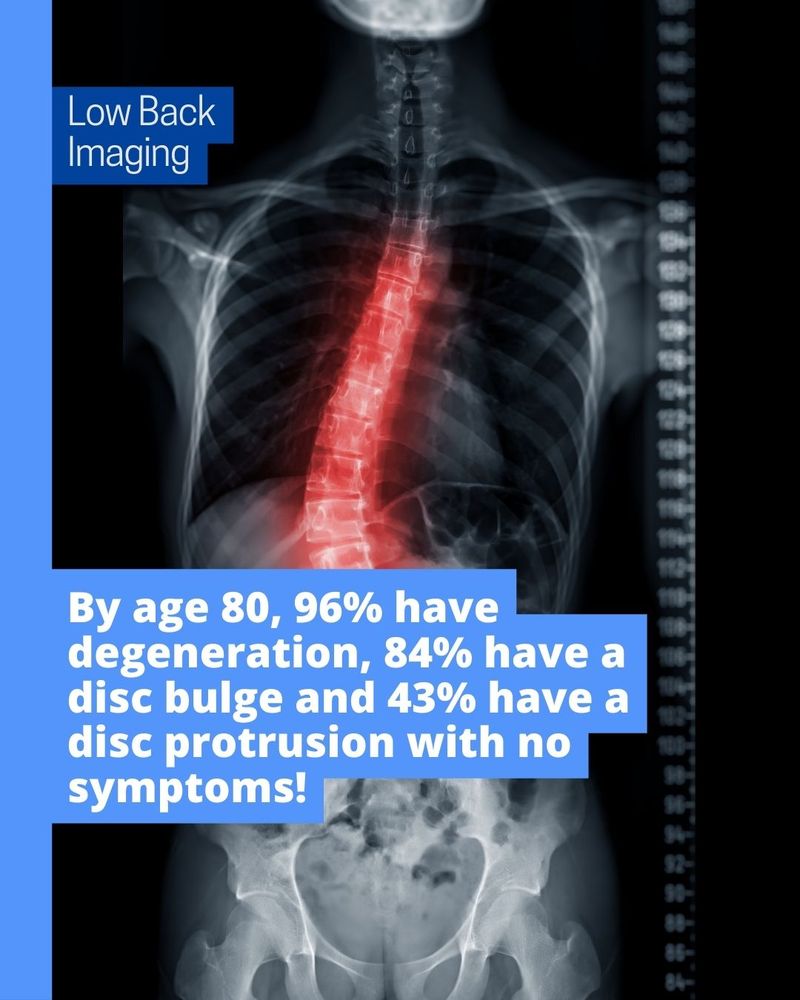
A study by Brinjikji et al. (2015) showed:
- By age 20: 37% had disc degeneration, 30% had a disc bulge, and 29% had a disc protrusion.
- By age 80: 96% had degeneration, 84% had a bulge, and 43% had a disc protrusion.
And these were people with no symptoms.
So, while imaging may look alarming, it doesn’t always correlate with pain. Two people with identical scan results can have completely different symptoms, movement restrictions, and recovery paths.
How Is Sciatica Diagnosed?
Sciatica is primarily diagnosed through a thorough history and physical examination in the clinic. Many people assume a scan is required to confirm the diagnosis, but that’s usually not the case unless there are red flags suggesting a more serious underlying condition (e.g. significant weakness, loss of bladder/bowel control, or unexplained weight loss).

What Triggers Sciatica?
A common belief is that sciatica starts after a clear event like heavy lifting. While this can be true, it’s more likely that symptoms appear spontaneously following a routine task you’d usually tolerate without issue like bending to pick something up.
This is because disc-related issues often build gradually over time. The disc weakens, and symptoms can seem to appear out of nowhere, not necessarily due to a single heavy lifting incident (Suri et al., 2010).
How Long Does Sciatica Last?
Recovery timelines vary, but here’s a rough guide based on research.
By 12 weeks, about 50% of people with sciatica fully recover, and by 12 months, approximately 70% do (Konstantinou et al., 2020).
However, like many forms of back pain, recurrence is common. Up to 1 in 4 people will experience a recurrence within a year, though it’s typically less severe than the first episode (Suri et al., 2012).
Functional Impact of Sciatica
Sciatica can affect daily activities like sitting, walking, lifting, and bending. Even normal movements such as twisting or getting out of a chair can become painful. The issue arises when these movements are labeled as “bad” or “dangerous,” which can create fear around movement. This fear often leads to avoidance, reduced activity, and eventually loss of function and deconditioning. When movement becomes something to fear, recovery slows down. It’s important to understand that pain does not always mean damage. Avoiding all activity may feel protective, but over time it can create more problems. Staying as active as your symptoms allow, and continuing to do tolerable forms of movement, is one of the best ways to support recovery.
After injury, it’s also normal to change how you move. If this becomes habitual with excessive bracing or avoiding any bending it can lower confidence and contribute to a cycle of fear. Building trust in your body again through gradual exposure to movement is key.
Role of Exercise in Recovery
It is common to hear that absolute rest is helpful after an injury, however, this is not the best option and is not recommended for many injuries especially back pain with sciatica (Vroomen, de Krom, Wilmink, Kester, & Knottnerus, 1999).
There are many benefits to maintaining some level of exercise in your daily life despite pain (such as maintaining your fitness level, creating less fear around movements and to show your body it is in fact capable of more than you think despite pain.
There are also risks to rest such as deconditioning, which initially may not become apparent, but, overtime when you do wish to restart exercise it is possible to do too much too soon after doing too little for too long which may lead to injury flare ups or a worsening of your condition.
This is why it’s important to enter rehab at a level that is suited to you and your injury. If you need help with managing your injury BOOK AN APPOINTMENT HERE!
Check out more Low Back Pain Myths here
References:
- Bogduk N. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain. 2009 Dec 15;147(1-3):17-9. doi: 10.1016/j.pain.2009.08.020. Epub 2009 Sep 16. PMID: 19762151.
- Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, Halabi S, Turner JA, Avins AL, James K, Wald JT, Kallmes DF, Jarvik JG. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015 Apr;36(4):811-6. doi: 10.3174/ajnr.A4173. Epub 2014 Nov 27. PMID: 25430861; PMCID: PMC4464797.
- Konstantinou K, Lewis M, Dunn KM, Ogollah R, Artus M, Hill JC, Hughes G, Robinson M, Saunders B, Bartlam B, Kigozi J, Jowett S, Mallen CD, Hay EM, van der Windt DA, Foster NE. Stratified care versus usual care for management of patients presenting with sciatica in primary care (SCOPiC): a randomised controlled trial. Lancet Rheumatol. 2020 Jun 25;2(7):e401-e411. doi: 10.1016/S2665-9913(20)30099-0. PMID: 32617529; PMCID: PMC7323615.
- Peng B, Wu W, Li Z, Guo J, Wang X. Chemical radiculitis. Pain. 2007 Jan;127(1-2):11-6. doi: 10.1016/j.pain.2006.06.034. Epub 2006 Sep 8. PMID: 16963186.
- Suri P, Hunter DJ, Jouve C, Hartigan C, Limke J, Pena E, Swaim B, Li L, Rainville J. Inciting events associated with lumbar disc herniation. Spine J. 2010 May;10(5):388-95. doi: 10.1016/j.spinee.2010.02.003. Epub 2010 Mar 29. PMID: 20347617; PMCID: PMC2919742.
- Suri P, Rainville J, Hunter DJ, Li L, Katz JN. Recurrence of radicular pain or back pain after nonsurgical treatment of symptomatic lumbar disk herniation. Arch Phys Med Rehabil. 2012 Apr;93(4):690-5. doi: 10.1016/j.apmr.2011.11.028. PMID: 22464091; PMCID: PMC3866041.
- Vroomen PC, de Krom MC, Wilmink JT, Kester AD, Knottnerus JA. Lack of effectiveness of bed rest for sciatica. N Engl J Med. 1999 Feb 11;340(6):418-23. doi: 10.1056/NEJM199902113400602. PMID: 9971865.

